
Whether you are navigating a diagnosis of ovarian cysts or endometriosis or you are considering preventive surgery due to high ovarian cancer risk, your care team may recommend an oophorectomy, a procedure to remove one or both ovaries.
At ESSE Care, we approach ovary removal thoughtfully. We do not remove ovaries unless medically necessary, because they play a vital role in hormone production and long-term health. If another provider recommends ovary removal without a clear explanation, that is a red flag. In these cases, we strongly encourage seeking a second opinion, and we’re happy to provide one.
What Is an Oophorectomy?

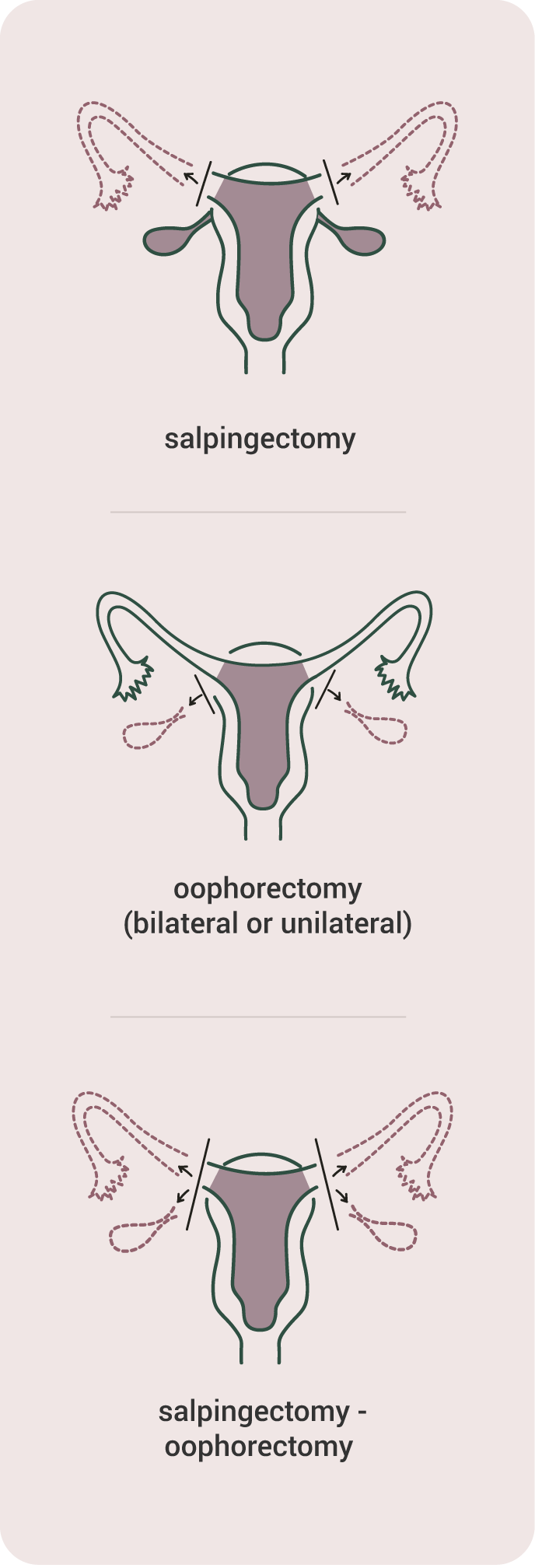
An oophorectomy is surgery to remove one (unilateral) or both (bilateral) ovaries. The ovaries are small, almond-shaped organs on each side of the uterus that store eggs and produce reproductive hormones like estrogen and progesterone.
This surgery may be performed on its own or alongside fallopian tube removal (salpingo-oophorectomy) or hysterectomy (removal of the uterus).
Common Myths About Oophorectomy
| Myth | Fact |
|---|---|
| Oophorectomy is just like having a hysterectomy. | Not exactly. A hysterectomy removes the uterus, but not necessarily the ovaries. Oophorectomy removes the ovaries, which has significant hormonal implications. |
| Oophorectomy always causes surgical menopause. | It depends. If one ovary remains and functions well, hormone production continues, and menopause should not occur immediately. |
| Ovary removal is standard during gynecologic surgery. | False. At ESSE, ovary removal is done only when medically necessary. Preserving the ovaries when it is safe is important for long-term health. |
How Oophorectomy Is Performed
Oophorectomy is most often performed as a same-day, outpatient procedure using minimally invasive techniques, such as laparoscopy or robotic-assisted surgery.
What to expect during an ovary removal procedure:
- Three to four small incisions (typically 5 to 8 mm) are made in the abdomen.
- A camera is inserted to visualize the pelvis.
- Specialized instruments are used to gently remove one or both ovaries.
- If part of your surgical plan, the fallopian tubes or uterus may also be removed.
- Incisions are closed with absorbable sutures.
Who Might Need This Surgery?
Oophorectomy may be recommended if you have:
- Large or complex ovarian cysts or tumors
- Recurrent endometriosis involving the ovaries, such as endometriomas
- Ovarian torsion, or twisting of the ovary
- Tubo-ovarian abscess or pelvic infection
- A genetic risk of ovarian or breast cancer, such as BRCA1 or BRCA2 mutations
- Confirmed ovarian cancer
At ESSE Care, we don’t typically recommend ovary removal to our patients when:
- Less invasive treatments can manage your condition, such as cystectomy or hormonal therapy.
- You are premenopausal and there is no confirmed cancer or high-risk genetic mutation.
- There are ovary-sparing options that are safe and effective.
Understanding Ovarian Cancer and Cancer Risk
Oophorectomy is sometimes recommended to treat ovarian cancer or lower cancer risk in individuals with certain genetic mutations or family history.
What Is Ovarian Cancer?
Ovarian cancer is a malignant tumor that develops from cells in the ovaries or fallopian tubes. Ovarian cancer can develop silently, with symptoms like bloating, pelvic pain, or changes in appetite often appearing late or not at all. Early detection is difficult, so risk-reduction strategies are important.
Who Is at Higher Risk of Developing Ovarian Cancer?
- Those with BRCA1 or BRCA2 mutations
- Strong family history of breast or ovarian cancer
- Certain inherited conditions, like Lynch syndrome
Risk-Reducing Surgery
For high-risk patients, removing the ovaries and fallopian tubes (bilateral salpingo-oophorectomy) can:
- Reduce ovarian cancer risk by up to 96%
- Lower breast cancer risk by up to 68% (if done before menopause)
This surgery is typically offered between ages 35 to 45, depending on your risk and reproductive plans. For some, fallopian tube removal (salpingectomy) alone may be an interim step to preserve fertility and avoid menopause before later ovary removal.
Red Flag: Ovary Removal Without Explanation
At ESSE Care, we believe ovary removal should be carefully justified. Even for women who no longer desire fertility, ovaries are essential for hormone balance, bone health, heart function, mood regulation, and metabolism. If a provider suggests removing your ovaries without clearly explaining why, particularly if you are premenopausal, it is important to seek a second opinion from a specialist with expertise in minimally invasive gynecologic surgery.
Preparing for Oophorectomy Surgery
Before your oophorectomy, your care team will help you prepare by:
- Reviewing your medications, including supplements and blood thinners
- Ordering imaging, such as ultrasound or MRI, to guide surgical planning
- Advising on when to stop eating or drinking before surgery
- Discussing fertility preservation, if appropriate
Make sure you have support at home for the first few days postoperatively. ESSE Care patients receive comprehensive support from our team to help you plan and prepare for your surgical procedure.
Oophorectomy Recovery and Aftercare
General Timeline
- Most patients go home the same day.
- Light walking and basic activities can usually resume immediately.
- Return to non-physical work typically occurs within 1 to 2 weeks.
- Sexual activity, heavy lifting, and core exercises should wait 4 to 6 weeks.
Post-Surgery Follow-Up
Patients typically return for a follow-up visit 1 to 2 weeks after surgery. During this appointment, we will assess incision healing, discuss symptom relief (including hormone therapy if needed), and review pathology results if any tissue was sent for biopsy.
How You May Feel After Oophorectomy Surgery
Physical healing is only one part of recovery. Many patients experience a range of emotions after oophorectomy. These may include:
- Fatigue or grogginess in the first few days
- Hot flashes, night sweats, or mood changes if both ovaries are removed
- Feelings of grief, sadness, or loss if fertility is affected
- Relief from symptoms such as chronic pelvic pain or cyst-related pressure
We encourage open conversation about how you are feeling. Emotional support and counseling are available, and we are here to help you navigate the physical and emotional aspects of healing.
Menopause and Hormonal Changes
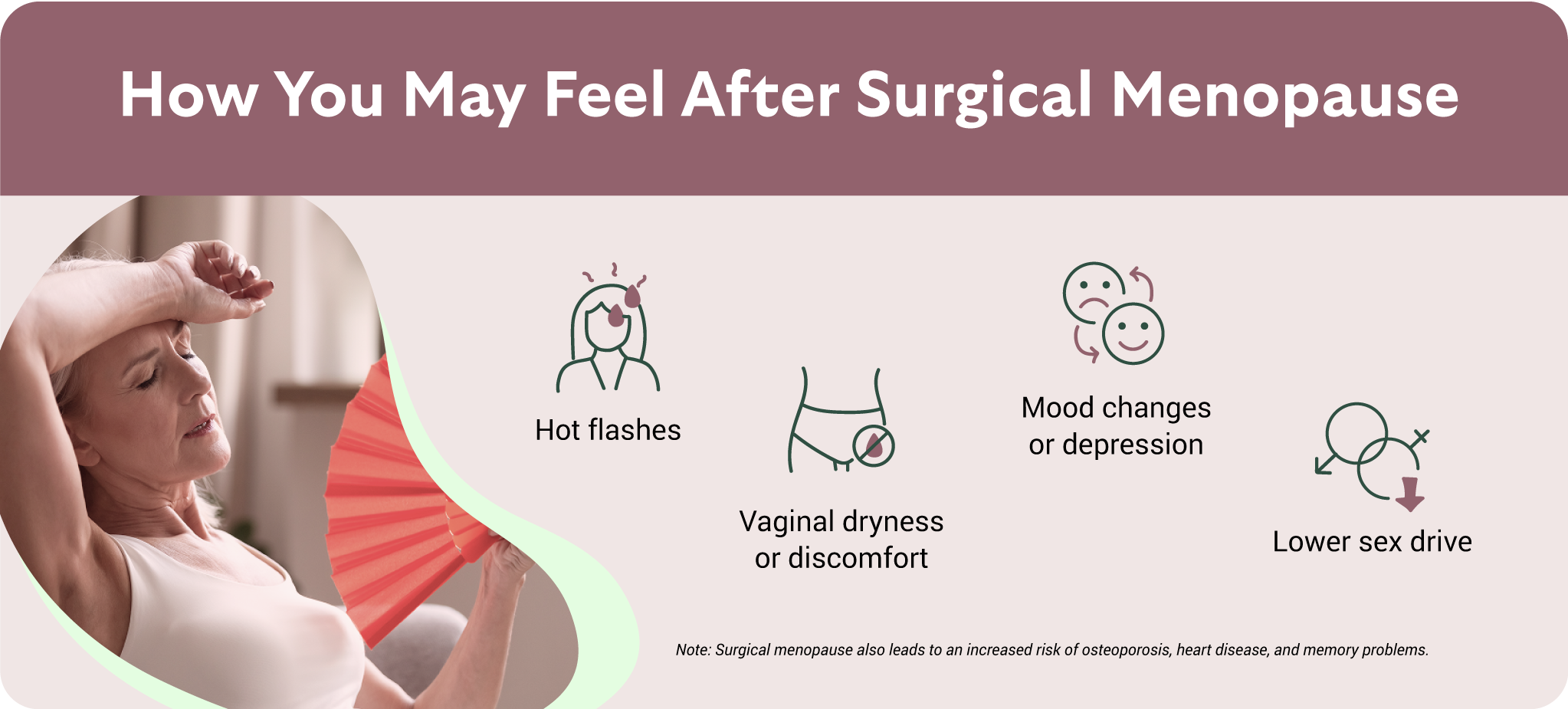
If both ovaries are removed, you will enter surgical menopause. This is a sudden drop in estrogen and progesterone, which can lead to symptoms and health risks such as:
- Hot flashes
- Vaginal dryness or discomfort
- Mood changes or depression
- Lower sex drive
- Increased risk of osteoporosis, heart disease, and memory problems
These risks are greater if you are under 45 years old. At ESSE Care, we consider the use of hormone replacement therapy (HRT) to reduce symptoms and protect long-term health. We will discuss the risks and benefits of HRT based on your age, health history (including conditions like endometriosis), and personal preferences.
Can You Get Pregnant After a Bilateral Oophorectomy?

A common question we hear from patients is whether pregnancy is possible after a bilateral oophorectomy. In the absence of both ovaries, pregnancy is no longer possible with your own eggs. The ovaries are responsible for producing both eggs and key reproductive hormones.
However, there are still options for building a family:
- Donor egg IVF: In this approach, a donated egg is fertilized and then transferred into your uterus if it is healthy and intact.
- Gestational surrogacy: Patients may consider this option if the uterus is not present or cannot safely carry a pregnancy.
- IVF with frozen eggs/embryos: If you are facing bilateral oophorectomy and hope to have children, we recommend speaking with a fertility specialist before surgery to see whether egg or embryo freezing may be an option.
- Embryo adoption: Did you know you may be able to adopt embryos? Many couples who successfully undergo IVF treatment decide to donate their unused embryos to prospective parents.
There are many paths to parenthood—even more than what we’ve listed here. Wherever your path leads, you don’t have to navigate it alone. At ESSE Care, we are here for you.
Note: While ESSE Care does not perform IVF, we work closely with top fertility centers to help support your reproductive goals and ensure coordinated care.
Helping You Navigate Your Oophorectomy Journey
At ESSE Care, we view surgery as one part of your larger care experience. We combine expert minimally invasive surgical techniques with compassionate, personalized care that considers your fertility, hormone health, and long-term wellness. If you are considering oophorectomy for a complex condition, cancer risk, or pain relief, our team is here to guide you with honesty and precision.
Schedule a consultation today to start the conversation.


