
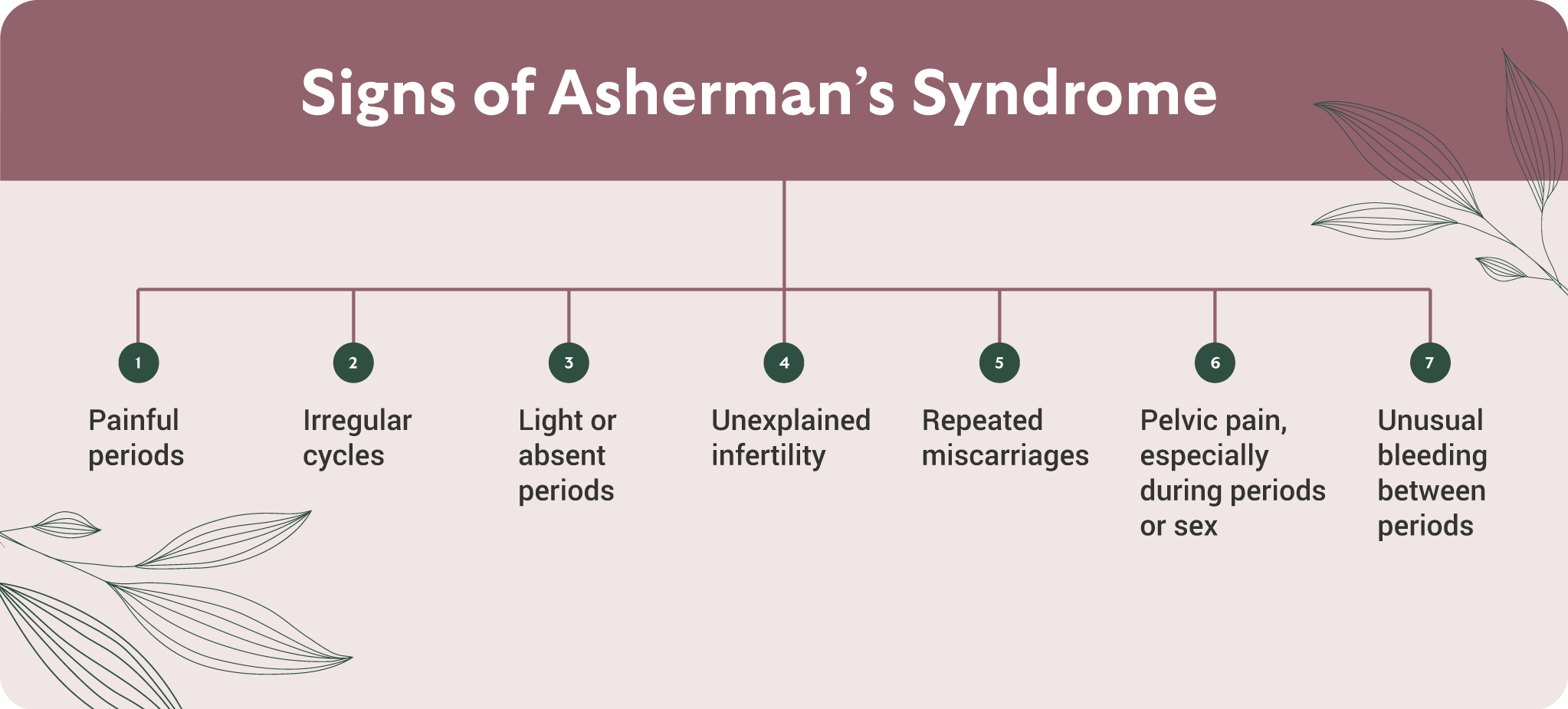
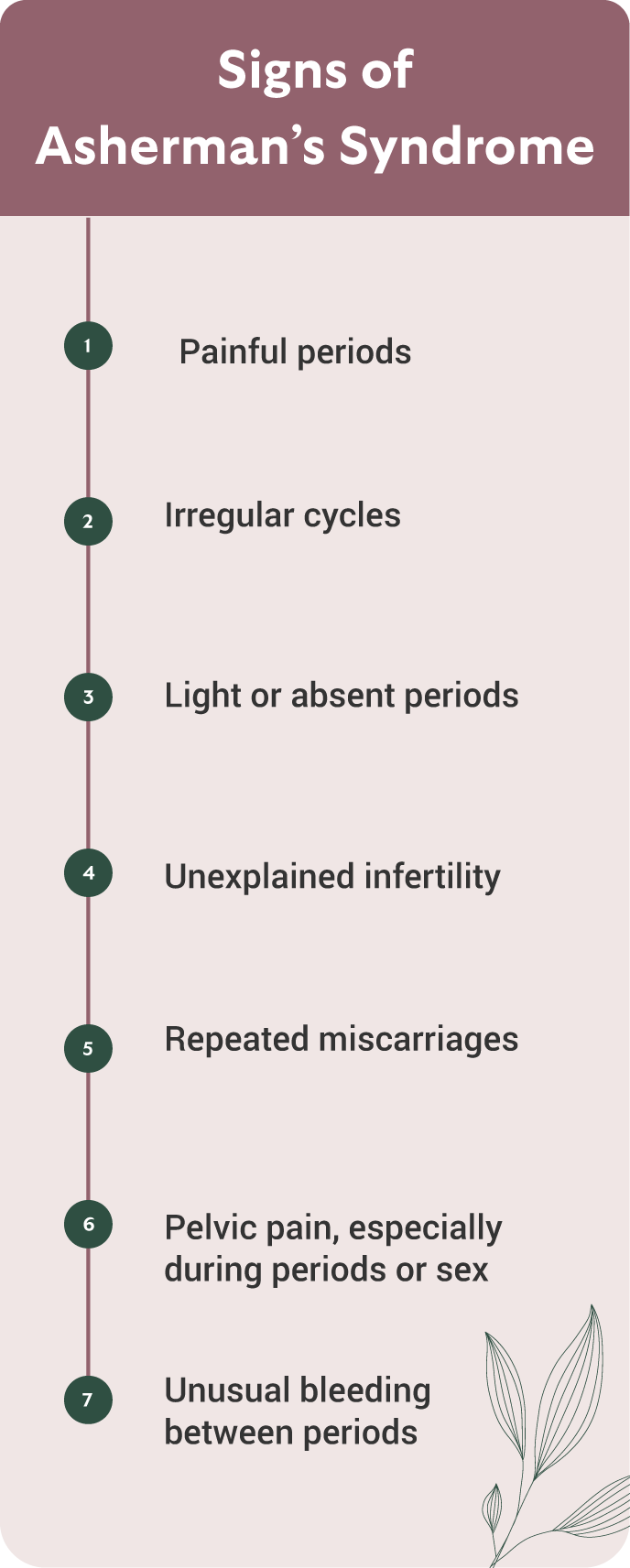
Scar tissue inside the uterus—called intrauterine adhesions, or Asherman’s Syndrome when severe—can interfere with fertility, disrupt menstrual flow, or cause pain during periods. It often forms after surgery or infection and may not be visible on routine imaging.
At ESSE Care, we use a gentle, minimally invasive approach to remove scar tissue hysteroscopically restoring the normal shape and function of the uterine cavity. This procedure can help you move forward in your path to healing with minimal disruption to your daily life.
What Is Hysteroscopic Adhesiolysis and How Is It Performed?
This procedure uses a hysteroscope, a small camera passed through the vagina and cervix into the uterus, to directly view and remove internal scar tissue. Here’s what happens, step by step:
- A hysteroscope is inserted through the cervix to visualize the inside of the uterus.
- Scar tissue is identified and gently removed using very fine scissors.
- In most cases, no heat or cautery is used to avoid further damage to the endometrium.
- A small balloon (Foley catheter) may be placed inside the uterus to prevent new scar tissue from forming.
- You may be given estrogen therapy and antibiotics after the procedure to support healing and reduce infection risk.
In cases of more complex or dense adhesions, a laparoscopy may be used to assist with visualization and safety. In this case, the surgeon will use several small abdominal incisions to insert the laparoscope (camera) and surgical tools. Laparoscopy is still a minimally invasive procedure.
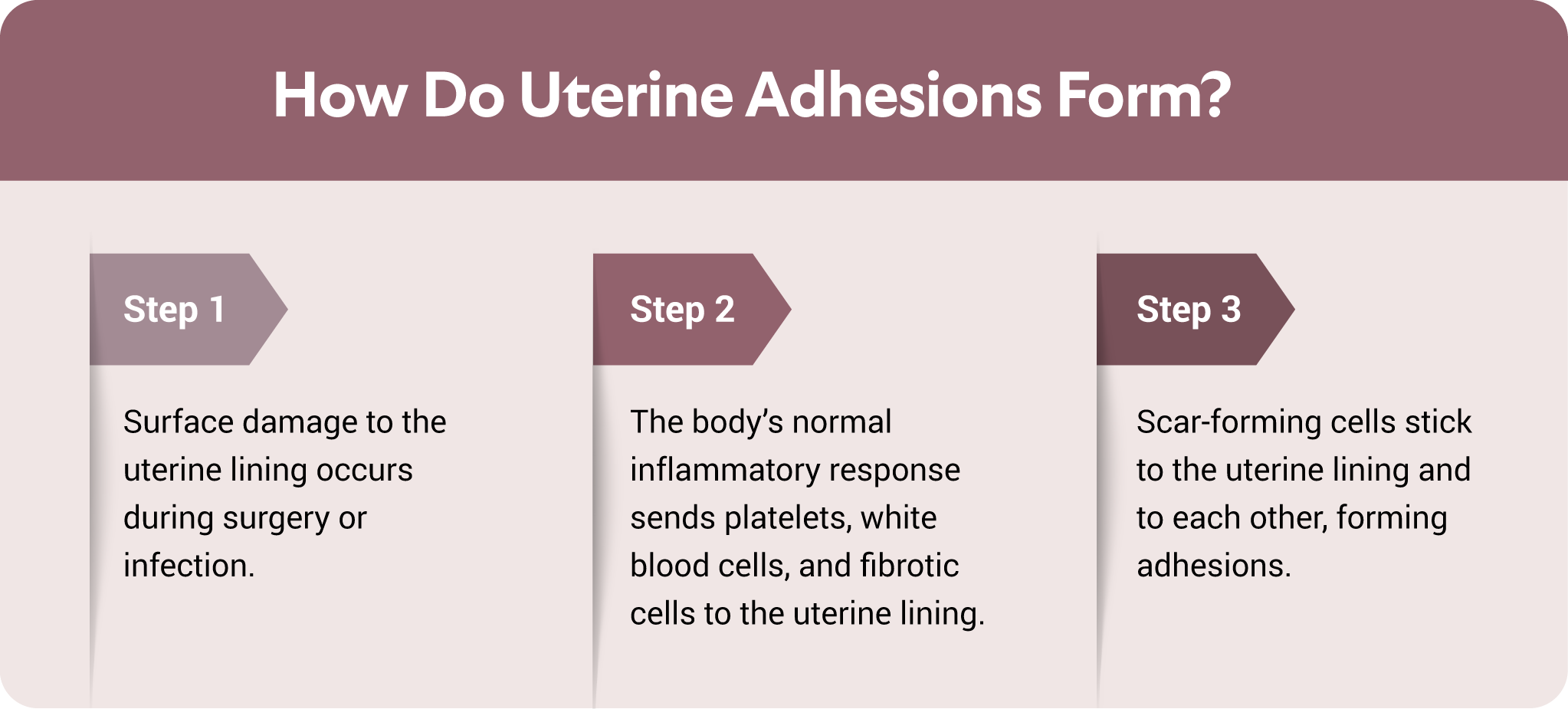
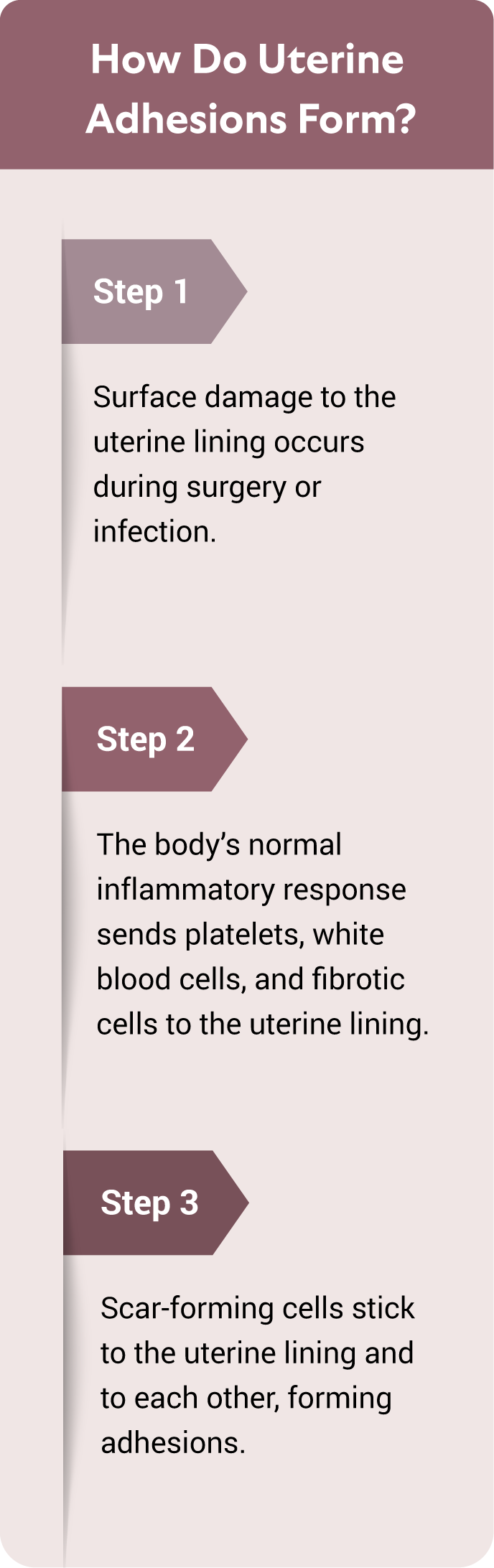
How Intrauterine Adhesions Form and Why They Matter
| Stage | What's Happening | Possible Symptoms or Consequences |
|---|---|---|
| 1. Injury to the uterine lining | Common after D&C, miscarriage management, retained placenta, or infections. | Often no immediate symptoms |
| 2. Scar tissue begins to form | The uterine walls may fuse together where injured. | Lighter periods, new cramps, or no bleeding at all |
| 3. Adhesions block or distort the uterine cavity | Blood can't flow normally, and embryo implantation is disrupted. | Infertility, miscarriages, or failed IVF cycles |
| 4. Chronic scarring limits endometrial regeneration | The uterine lining may become thin, patchy, or nonfunctional. | Persistent infertility, complications in pregnancy (e.g., adherent placenta) |
Who Might Need This Surgery?
You may be a candidate for hysteroscopic lysis of adhesions if you:
- Are trying to conceive and have been diagnosed with uterine scarring
- Have experienced a significant drop in menstrual flow or painful periods after surgery or infection
- Are undergoing fertility evaluation and imaging suggests a distorted uterine cavity, fluid buildup, or a thin uterine lining
- Have been diagnosed with Asherman’s syndrome via saline sonogram or hysterosalpingogram (HSG)
When It Might Not Be Recommended
Not all scar tissue needs to be removed. If you are not experiencing symptoms and are not trying to get pregnant, or if imaging shows very minimal or incidental scarring, you may not require surgery at all.
Recovery and Aftercare for Hysteroscopic Adhesiolysis
Same-Day Procedure, Smooth Recovery
- Most patients go home the same day
- The procedure itself is typically under an hour
- Cramping and light bleeding are common for a few days
- Tylenol or Advil is usually sufficient for pain relief
- You may be prescribed hormonal medication (often estrogen) and antibiotics post-op
Activity Guidelines
- Return to light activity/work: The next day
- Full internal healing: Usually one menstrual cycle (4–6 weeks)
- Activity restrictions:
- No intercourse, tampons, menstrual cups, baths, or swimming for 2 weeks
- No lifting or exercise restrictions unless you are uncomfortable with the intrauterine balloon
Risks and Complications
Most patients recover well, but some of the risks include but are not limited to:
- Uterine perforation
- Recurrence of scar tissue (especially with severe Asherman’s syndrome)
- Adherent or abnormal placenta in future pregnancy
Long-Term Considerations
If you have symptoms and decide to forego surgery, scar tissue may remain and continue to interfere with:
- Fertility
- Menstrual regularity
- Embryo implantation
Success Rates and Long-Term Outlook
- Effectiveness: Most patients see significant improvement in uterine shape and function after adhesions are removed
- Recurrence: More likely with severe or longstanding adhesions, but less common after mild cases
- Fertility outcomes: Improve significantly when the cavity can be fully restored
- Repeat procedures: May be needed in some cases, especially with severe scarring, but our team will only recommend another surgery if meaningful progress is expected
Preparing for Hysteroscopic Lysis of Intrauterine Adhesions
Pre-operative testing may include:
- Saline sonogram, hysterosalpingogram (HSG), or MRI to visualize the uterine cavity
- Routine labs
- Medication adjustments (your care team will guide you)
Post-Surgery Support
Follow-up care for hysteroscopic adhesiolysis includes:
- Balloon (Foley) removal around 7 days post-op (if used)
- Post-op visit with your surgeon to review your healing and symptoms
- Repeat imaging (sonogram or hysteroscopy) to confirm cavity restoration
Your Surgical Journey at ESSE Care
We know that Asherman’s syndrome and uterine scarring can be overwhelming—especially if you’ve been experiencing uncomfortable symptoms or navigating infertility. At ESSE Care, we take a gentle, thorough approach focused on restoring uterine function and supporting your long-term reproductive health.
You can expect:
- Thoughtful, evidence-based evaluation of your uterine health
- Minimally invasive care with precision and compassion
- Collaborative planning with fertility specialists and obstetricians
- Post-surgery support, including imaging and recommendations for complementary therapies
If you’ve been diagnosed with intrauterine adhesions or are experiencing symptoms that don’t make sense, we’re here to help. Schedule a consultation with the ESSE Care team to explore if hysteroscopic scar tissue removal is the next right step for you.


