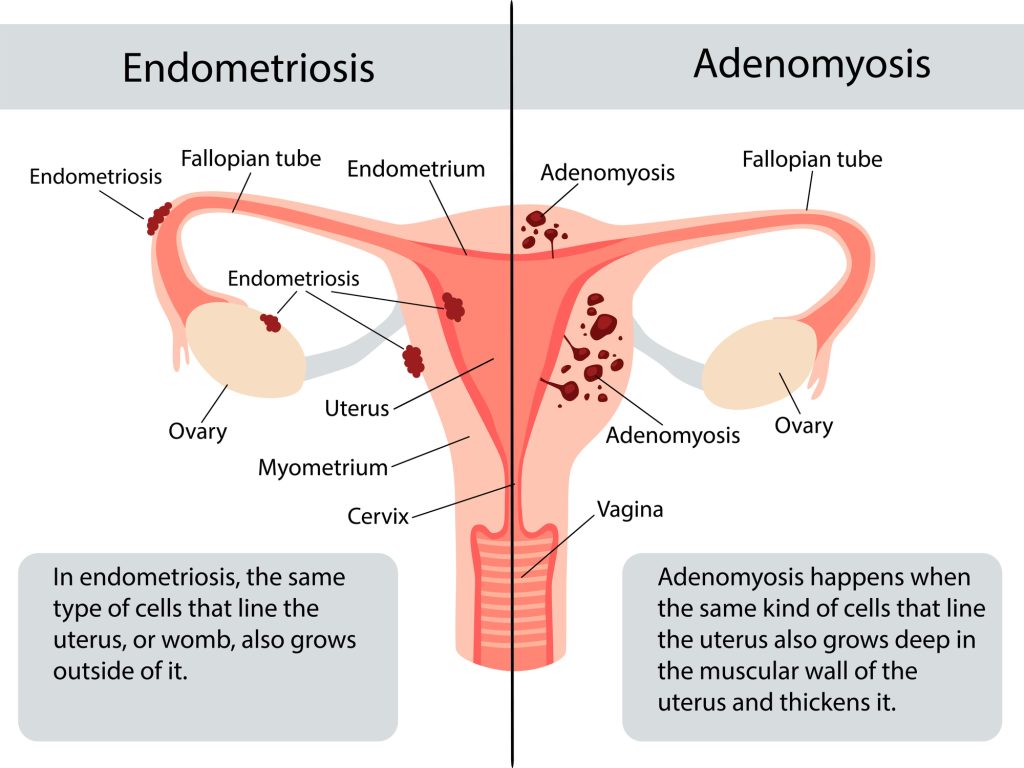
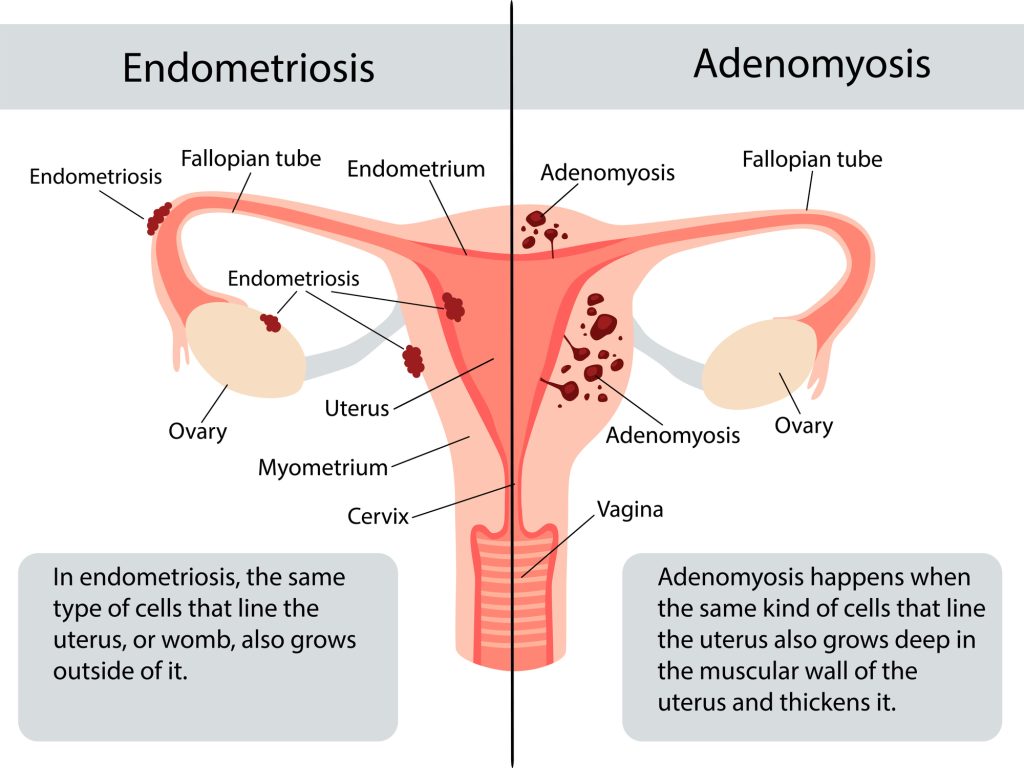
Adenomyosis is often described as the sister disease of endometriosis. Adenomyosis often occurs hand in hand with endometriosis but some patients may have one without the other. Adenomyosis is when glands or stromal cells similar to those in the endometrial cavity grow within the uterine walls.
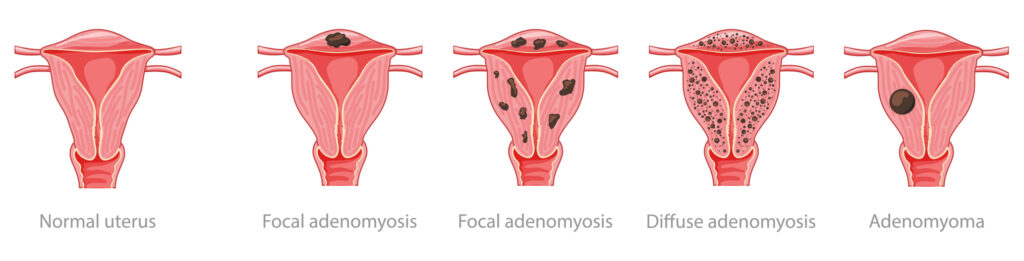
It is best seen in the cartoons below.
Adenomyosis can cause extremely painful periods, very severe debilitating cramping with heavy clots, and heavy menstrual bleeding. Patients may miss school or work in the days leading up to the period- often the cramping is strongest those days before to the first 2 days of cycle.
Adenomyosis can be diffuse where there are multiple small cystic regions in the wall of the uterus that over time cause the uterus to be thickened and bulky (often on one wall of the uterus more than the other i.e. posterior/back wall of uterus or front wall anterior).
Adenomyoma refers to a singular fibroid-like mass that is concentrated like a fibroid nodule. Unfortunately, adenomyosis and adenomyomas are not typically in a nice shell like a fibroid. This means they frequently have irregular borders and tentacle-like infiltration around them into the myometrial or uterine muscle walls.
This makes it harder to remove them, and the tissue surrounding them is fibrotic and inflamed causing more difficult repair technically. (Suture may pull and shred the muscle layer easily because it is poor tissue strength over time from the disease).
This is in stark contrast to typical fibroid removal surgery or myomectomy where the uterine walls aside from the fibroid itself are healthy. They are easier to approximate with suture, and the suture or stitching typically holds very well following.
For this reason, adenomyosis removal should be undertaken with extreme caution especially in a patient who desires pregnancy or to carry with the uterus following.
The recommended wait time post adenomyomectomy to get pregnant after myomectomy or adenomyosis removal is 3-6 months. We recommend at least 6 months. And very careful consideration in pregnancy or if pregnancy is desired.
Dr Goldstein will review your particular case and the uterine anatomy and discuss your desires for the future for fertility. Often adenomyosis maybe left in place and suppressed with success pre-pregnancy and removal maybe deferred until after child bearing.
Everything is done on a case-by-case basis to determine the best plan for you and your fertility interests.
While the definitive treatment for adenomyosis is hysterectomy or removal of the uterus, adenomyosis can be managed until that time is desired.