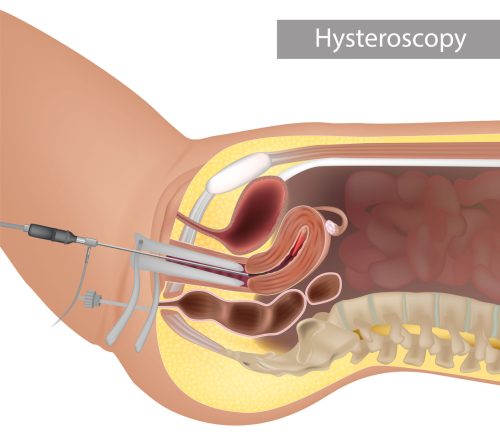
Hysteroscopy means a camera inserted in the vagina, into the cervix and then into the uterine cavity. This can be performed with ease by inserting the camera vaginally “touchless” if the cervix is already pre-dilated (vaginoscopy) and inserting directly into the cervix. By performing hysteroscopy like this we can see the actual angle an embryo transfer would occur (how steep the cervix angle is to the cavity). This can be performed with photos so your fertility doctor can see them in the future.
If the uterus or cavity has abnormalities in it from prior surgery like an isthmocele this technique can greatly aid in seeing the angle and anatomical distortions or problems.
After hysteroscopy the cervix is maximally dilated and different special testing can be performed like CD138 for chronic endometritis or infection/inflammation which could affect implantation or miscarriage.
Endometrial scratch or gentle curettage can be performed to help insure the next endometrial lining is thick for the possible implantation or pregnancy. If you have had a difficult or painful embryo transfer it maybe related to the uterine angle if it is severely tilted backwards or retroverted. In this case the uterus can be temporarily lifted with suspension or shortening of the round ligaments. (Round ligament plication).
For patients with a history of painful intercourse/ultrasound or difficult transfer this could greatly benefit them in the future.
The suture placed is temporary but we think reinforces the integrity of the ligaments and eases discomfort in the future.
Septum excision can be performed for correction of significant septum/arcuate uterus in patients with miscarriage, failed embryo transfer or other indications. This can also relieve dysfunctional uterine bleeding in patients with dark clots/ irregular menstrual bleeding.
Advanced septum excision for patients with vaginal septum and intrauterine septum can be performed with concurrent vaginoscopy.










